
Is Meloxicam Stronger Than Over-the-Counter Pain Meds?
By Frankie Sze| 5/2/2026
The ‘Strength’ Misconception: Intensity vs. Duration
When patients inquire about analgesic potency, the term ‘stronger’ is frequently misinterpreted to mean how rapidly a medication quells an acute flare-up. This expectation is largely a legacy of the 1980s, when ibuprofen became the gold standard for over-the-counter pain management, establishing a public consensus that ‘strength’ equates to the speed of onset—usually within 30 to 60 minutes. However, in a clinical context, a medication’s superiority often hinges on pharmacokinetics rather than immediate impact. As noted by Drugs.com, “Meloxicam is considered a stronger medicine than ibuprofen,” a claim rooted in its milligram-for-milligram potency, which is roughly 10 to 20 times that of ibuprofen.
The fundamental distinction lies in the temporal profile of these drugs. Ibuprofen is characterized by a short half-life of two to four hours, necessitating frequent dosing to maintain therapeutic levels. In contrast, meloxicam boasts a terminal half-life of 15 to 20 hours, allowing for once-daily administration. For those managing chronic conditions like arthritis, this provides a more consistent baseline of relief, as the drug reaches steady-state plasma concentrations after only three to five days of regular use. To understand how this impacts your long-term management strategy, explore our Meloxicam 101: Your Daily Guide to Steady Joint Relief. Beyond duration, meloxicam’s preferential selectivity for the COX-2 enzyme—which is linked to a reduced risk of gastrointestinal complications compared to non-selective NSAIDs—marks a significant shift in clinical practice. While researchers continue to investigate how further COX-2 selectivity might mitigate cardiovascular and renal risks, physicians currently prioritize meloxicam to improve patient adherence, successfully reframing ‘strength’ from a burst of intensity to the reliability of steady, sustained care.

The Science of Persistence: How Half-Life Redefines Strength
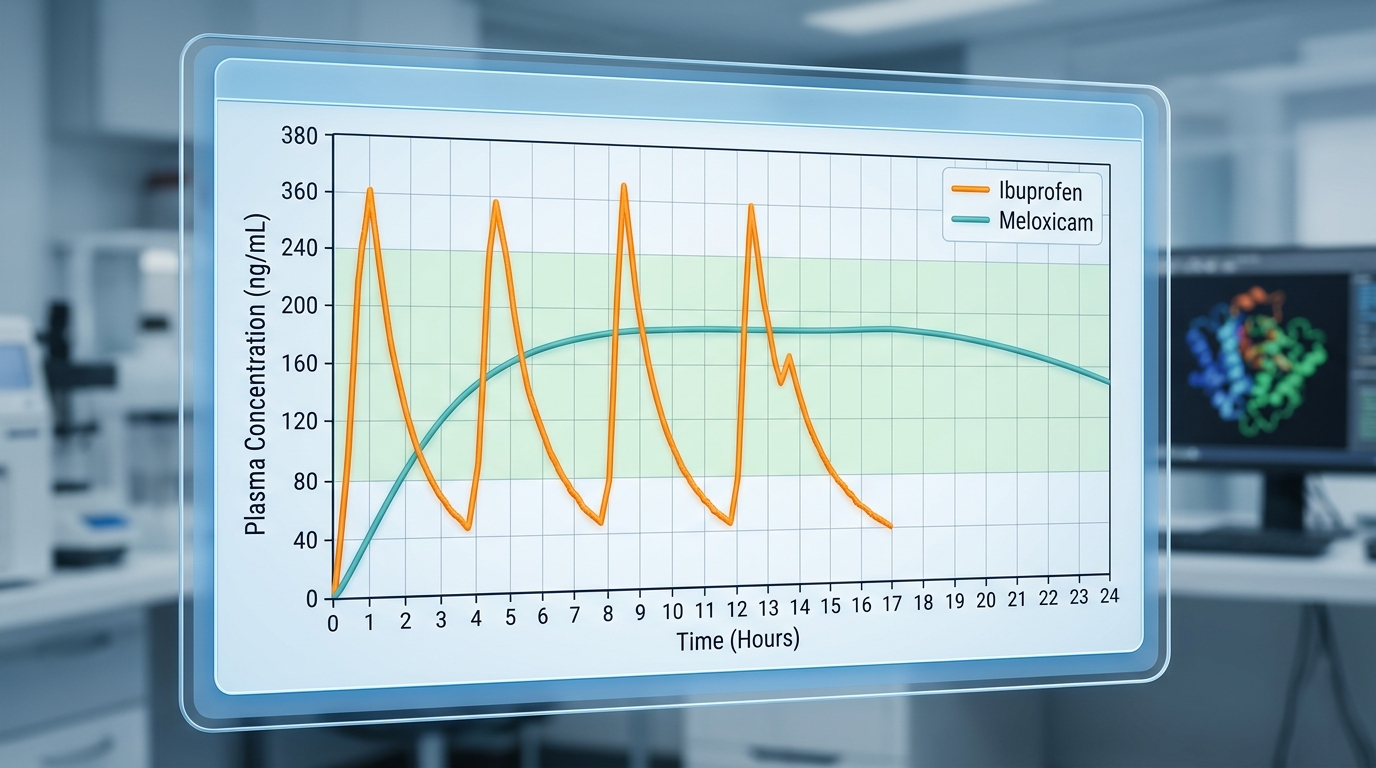
Since ibuprofen became the over-the-counter standard for acute pain in the 1980s, patients have developed a reflexive expectation that medication strength is measured by the speed of its onset. Ibuprofen typically delivers relief within 30 to 60 minutes; however, its pharmacological profile is defined by a short terminal half-life of only 2 to 4 hours. This rapid clearance necessitates frequent dosing every 4 to 6 hours to sustain therapeutic levels, which can lead to gaps in pain management and challenges with patient adherence. In contrast, meloxicam represents a shift toward sustained efficacy. As a 15 mg dose of meloxicam is approximately 10 to 20 times more potent on a milligram-for-milligram basis than ibuprofen, its mechanism of action is both more concentrated and prolonged. With a terminal half-life of 15 to 20 hours, meloxicam avoids the ‘peaks and valleys’ of short-acting NSAIDs. According to The Freedom Center, “Its longer half-life means the medication stays active throughout the day, providing consistent pain relief.”
This pharmacokinetic stability allows meloxicam to reach steady-state plasma concentrations after 3 to 5 days of once-daily dosing, a convenience that has led physicians to increasingly prioritize it for chronic arthritis management. Beyond the convenience of a single daily pill, meloxicam’s preferential selectivity for the COX-2 enzyme offers a critical clinical advantage, as this pathway is associated with fewer gastrointestinal side effects than non-selective NSAIDs. While we look toward a future where ongoing research into COX-2 selectivity seeks to further mitigate the cardiovascular and renal risks of long-term use, the current standard for persistent pain lies not just in the speed of the relief, but in the reliability of the steady state.
Potency at the Source: Meloxicam’s Concentration in Joint Fluid
For patients navigating the persistent discomfort of chronic arthritis, the definition of effective pain management has shifted from the rapid-onset, short-acting relief exemplified by the 1980s standard of ibuprofen to a focus on sustained, localized efficacy. While ibuprofen remains a staple for acute pain—typically providing relief within 30 to 60 minutes due to its short half-life of 2 to 4 hours—it requires frequent dosing that can challenge patient adherence. In contrast, meloxicam offers a more consistent profile for chronic conditions. As noted in clinical analysis, “Meloxicam achieves therapeutic concentrations in the joint space that are maintained for a full 24 hours after a single oral dose of 7.5 mg–15 mg.”
This pharmacokinetic stability is driven by meloxicam’s terminal half-life of 15 to 20 hours, allowing for once-daily dosing that reaches steady-state plasma concentrations after just 3 to 5 days. Beyond its temporal advantages, meloxicam exhibits superior potency; on a milligram-for-milligram basis, a 15 mg dose is approximately 10 to 20 times more potent than ibuprofen. Furthermore, because meloxicam is preferentially selective for the COX-2 enzyme, it offers a distinct advantage for long-term users by significantly reducing the risk of gastrointestinal side effects often associated with non-selective NSAIDs. By concentrating effectively within the synovial fluid, meloxicam ensures that the patient’s joints remain protected against inflammatory markers throughout the entire day, bridging the gap between momentary symptom management and sustained therapeutic control.
Selective Targeting: Why COX-2 Selectivity Feels ‘Stronger’ for Arthritis
While ibuprofen became the over-the-counter standard for acute pain in the 1980s, establishing a public expectation that “strength” is synonymous with immediate, short-lived relief, the management of chronic arthritis demands a different pharmacological profile. In this context, meloxicam offers a more refined approach to inflammation. By acting preferentially on the COX-2 enzyme—which is primarily induced at sites of injury—meloxicam minimizes the collateral inhibition of COX-1, an enzyme responsible for protective gastric functions. As noted by experts, “Meloxicam targets the COX-2 enzyme, reducing inflammation and pain with fewer stomach side effects than many traditional NSAIDs” (AMSK Insights).
This selectivity is bolstered by pharmacokinetic advantages that favor consistent, long-term therapeutic control over sporadic dosing. Whereas ibuprofen has a short terminal half-life of only two to four hours, necessitating frequent ingestion, meloxicam boasts a half-life of 15 to 20 hours. On a milligram-for-milligram basis, a 15 mg dose of meloxicam is approximately 10 to 20 times more potent than ibuprofen, allowing it to reach a steady-state plasma concentration within three to five days of once-daily use. For patients managing chronic joint stiffness, this consistency significantly improves adherence compared to the rapid-acting but fleeting cycle of traditional NSAIDs. As medical science evolves, ongoing research into COX-2 selectivity seeks to further refine these outcomes, aiming to mitigate the cardiovascular and renal risks that have historically accompanied long-term anti-inflammatory therapy.
The Speed Trade-off: Why Stronger Isn’t Always Faster
In the world of analgesics, public perception has long been shaped by the 1980s shift toward ibuprofen as the over-the-counter gold standard for acute pain, fostering a persistent belief that a medication’s “strength” is synonymous with its speed of action. However, clinicians recognize a distinct pharmacological divide between potency and onset. Ibuprofen remains the superior choice for immediate relief, typically providing acute pain management within 30 to 60 minutes of ingestion. As noted by experts at The Freedom Center, “You’ll typically feel relief within 30-60 minutes.” Because ibuprofen possesses a short terminal half-life of only 2 to 4 hours, it necessitates frequent dosing every 4 to 6 hours to maintain its therapeutic window, which is ideal for the transient nature of a tension headache or sudden injury.
Conversely, meloxicam is designed for a different clinical landscape: chronic, systemic inflammation. While a 15 mg dose of meloxicam is roughly 10 to 20 times more potent on a milligram-for-milligram basis than ibuprofen, this strength does not translate to immediate relief. Meloxicam is preferentially selective for the COX-2 enzyme—a profile that offers fewer gastrointestinal side effects compared to non-selective agents—but it requires a longer metabolic ramp-up. With a terminal half-life of approximately 15 to 20 hours, meloxicam reaches steady-state plasma concentrations only after 3 to 5 days of consistent, once-daily dosing. This gradual approach is why doctors increasingly prescribe it for chronic arthritis; the extended duration of action improves patient adherence, even if it cannot compete with the rapid-fire onset of traditional acute-care NSAIDs. Looking toward the future, ongoing research into COX-2 selectivity aims to further refine this balance, seeking to mitigate the cardiovascular and renal risks currently associated with the long-term use of such potent therapies.
Making the Choice: When Prescription Control Outperforms OTC
For decades, the over-the-counter dominance of ibuprofen has cemented a public perception that therapeutic ‘strength’ is synonymous with rapid onset. While ibuprofen serves as an excellent tool for acute pain—typically providing relief within 30 to 60 minutes—its short half-life of 2 to 4 hours necessitates frequent, disruptive dosing. In contrast, clinical decision-making for chronic inflammatory conditions increasingly favors the consistent pharmacological profile of meloxicam. As noted in expert clinical analysis, “Meloxicam excels for chronic inflammatory conditions like rheumatoid arthritis requiring consistent relief throughout the day and night.”
This clinical preference is rooted in the drug’s unique pharmacokinetic properties. With a terminal half-life of 15 to 20 hours, meloxicam allows for once-daily dosing, which significantly improves patient adherence. On a milligram-for-milligram basis, a 15 mg dose of meloxicam is approximately 10 to 20 times more potent than ibuprofen, and it achieves steady-state plasma concentrations after just 3 to 5 days of use. Beyond its consistent coverage, meloxicam’s preferential selectivity for the COX-2 enzyme offers a favorable profile regarding gastrointestinal side effects compared to non-selective agents. Readers interested in the transition from intermittent relief to a sustained management strategy can explore Meloxicam 101: Your Daily Guide to Steady Joint Relief. As we look toward the future, ongoing research into COX-2 selectivity aims to further refine these prescription options, balancing long-term efficacy with cardiovascular and renal safety to ensure that chronic pain management remains both effective and sustainable.


