Speed vs. Staying Power: Meloxicam vs. Ibuprofen Timing
By Frankie Sze| 5/2/2026
The Sprint vs. The Marathon: Introduction to NSAID Timing
In the landscape of pain management, not all non-steroidal anti-inflammatory drugs (NSAIDs) are created equal. While both ibuprofen and meloxicam serve to reduce pain and inflammation, their ‘pharmacokinetic personalities’ dictate fundamentally different roles in patient care. As noted by The Freedom Center, “Meloxicam and ibuprofen are both NSAIDs that reduce pain and inflammation, but meloxicam is prescription-only while ibuprofen is available over-the-counter.”
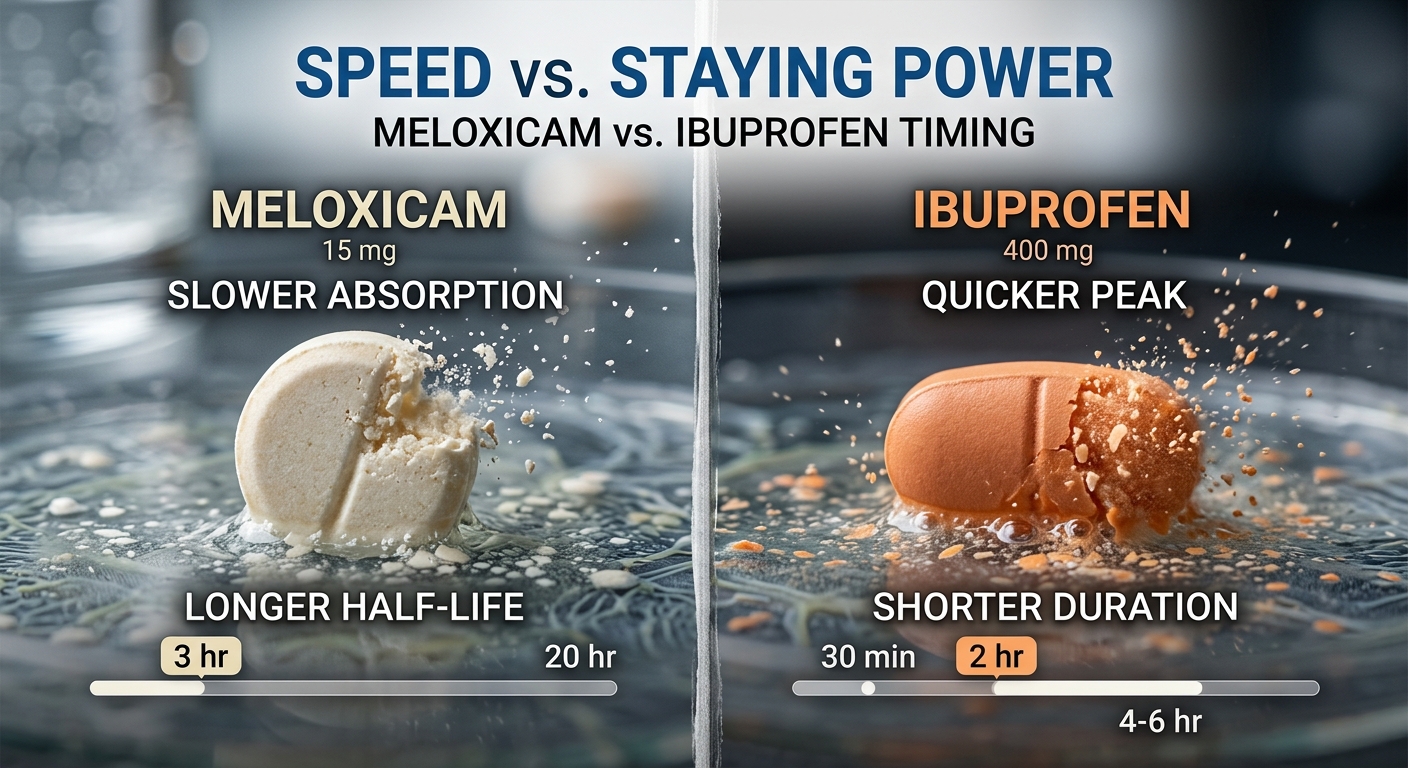
Ibuprofen functions as the clinical ‘sprinter.’ It has long been the gold standard for acute pain due to its rapid onset, typically providing relief within 30 to 60 minutes. However, its effects are transient, lasting only 4 to 6 hours, which necessitates frequent dosing. In contrast, meloxicam serves as the ‘marathon runner,’ specifically developed to address the need for consistent, once-daily coverage in chronic inflammatory conditions like arthritis. Because meloxicam has an elimination half-life of approximately 20 hours and reaches steady-state plasma concentrations within 3 to 5 days, it provides a stable therapeutic baseline that improves patient adherence.
Clinicians must recognize these distinct temporal profiles before treatment. While ibuprofen reaches its peak quickly, meloxicam reaches peak plasma concentration (Tmax) in 5 to 6 hours, with some oral formulations taking up to 11 hours to reach full effect. Because meloxicam is preferentially selective for COX-2, it may offer reduced stomach irritation compared to non-selective agents like ibuprofen; however, patients must be warned against combining these medications, as the synergy significantly increases the risk of stomach ulcers, gastrointestinal bleeding, and kidney damage. For a deeper look at the transition to long-term care, our guide Meloxicam 101: Your Daily Guide to Steady Joint Relief details how to manage this transition safely. Regardless of the chosen path, ongoing monitoring for cardiovascular and kidney health remains essential, with a continuous mandate to reassess dosing to ensure the lowest effective dose is used for the shortest possible duration.

Ibuprofen: The Rapid-Response Specialist for Acute Pain
For patients navigating sudden-onset discomfort, ibuprofen remains a cornerstone of acute pain management due to its predictable and swift pharmacokinetics. As a non-selective NSAID, it is designed for ‘right now’ relief, and clinical consensus highlights that, as noted by The Freedom Center, “You’ll typically feel relief within 30-60 minutes.” This rapid onset makes it the preferred choice for headaches, minor injuries, or acute flares where immediate intervention is required.
However, this therapeutic speed comes with a significant logistical trade-off: the need for frequent dosing. The effects of standard ibuprofen typically last only 4-6 hours, requiring patients to remain vigilant about their administration schedule to maintain therapeutic efficacy. This is in stark contrast to medications like meloxicam, which were developed to address the needs of chronic inflammatory conditions through once-daily dosing. While meloxicam offers the convenience of 24-hour coverage, it possesses a much slower onset, with peak plasma concentrations (Tmax) taking 5-6 hours—or up to 11 hours depending on the formulation—and an elimination half-life of approximately 20 hours. Given these distinct pharmacokinetic profiles, clinicians must weigh the immediate, short-acting utility of ibuprofen against the sustained, steady-state benefits of once-daily alternatives.

Meloxicam: Engineering All-Day Steady-State Relief
While ibuprofen has long served as the standard for acute pain management due to its rapid onset of 30 to 60 minutes, its therapeutic window is brief, typically lasting only 4 to 6 hours. This necessitates frequent dosing, which often complicates long-term management for patients dealing with persistent inflammation. In contrast, meloxicam was specifically engineered to address the practical limitations of such frequent administration. With an elimination half-life of approximately 20 hours, meloxicam provides a more stable therapeutic profile, allowing patients to achieve steady-state plasma concentrations within 3 to 5 days of once-daily dosing. As noted by The Freedom Center, “Meloxicam offers once-daily dosing with longer-lasting effects, making it preferred for chronic inflammatory conditions like arthritis.”
The pharmacological design of meloxicam offers significant advantages for patient adherence. Although the medication reaches peak plasma concentration (Tmax) in 5 to 6 hours—with some formulations extending up to 11 hours—the goal is not immediate relief, but rather consistent, 24-hour coverage. Furthermore, meloxicam’s preferential selectivity for the COX-2 enzyme may mitigate some of the gastric irritation associated with non-selective NSAIDs like ibuprofen. However, clinical vigilance remains paramount; clinicians must emphasize that combining meloxicam with other NSAIDs like ibuprofen significantly elevates the risk of gastrointestinal bleeding, stomach ulcers, and renal impairment. As we move toward the future of pain management, ongoing monitoring for cardiovascular and kidney health remains a standard of care, ensuring that every patient is prescribed the lowest effective dose for the shortest necessary duration.
The Wait for Results: Why Meloxicam Often Takes Days to Reach Full Strength
For patients accustomed to the immediate relief provided by standard ibuprofen—which typically acts within 30 to 60 minutes—beginning a course of meloxicam requires a shift in expectations. While ibuprofen is a rapid-acting intervention with a short duration of effect, lasting only 4 to 6 hours, meloxicam was specifically engineered for chronic inflammatory conditions requiring consistent, long-term management. Because meloxicam has an elimination half-life of approximately 20 hours, it is designed for once-daily dosing to maintain stable therapeutic levels, rather than the quick, episodic peaks associated with other NSAIDs.
Patients should understand that meloxicam does not function like a “rescue” medication. While it reaches peak plasma concentration (Tmax) in 5 to 6 hours—though some oral formulations may require up to 11 hours—full therapeutic efficacy is a cumulative process. According to clinical research, “Steady state is achieved within 3 to 5 days” of consistent, once-daily dosing. This period of accumulation is critical for the drug to stabilize in the bloodstream and effectively manage inflammation.
It is tempting for patients to supplement with ibuprofen during this initial window, but this must be avoided. Combining meloxicam with ibuprofen significantly increases the risk of gastrointestinal complications, including stomach ulcers and bleeding, as well as potential kidney damage. While meloxicam is preferentially selective for the COX-2 enzyme—which generally offers a better profile for stomach irritation compared to non-selective NSAIDs—that protection is negated when additional NSAIDs are introduced. If you do not feel 100% relief in the first hour, avoid the urge to self-medicate with other anti-inflammatories; trust the steady-state process, and if symptoms remain unmanaged after the initial five-day window, consult your clinician to ensure you are on the lowest effective dose for your specific condition.
Clinical Trade-offs: Choosing Speed or Endurance Based on Pain Type
When managing pain, the clinical decision often hinges on the temporal nature of the symptoms: immediate onset versus persistent inflammation. Ibuprofen remains the gold standard for acute pain, such as episodic headaches, largely due to its rapid pharmacokinetic profile. It typically provides relief within 30 to 60 minutes, though this effect is transient, lasting only 4 to 6 hours. Conversely, chronic inflammatory conditions like arthritis demand consistent therapeutic coverage. Meloxicam was specifically developed to address this need, utilizing a longer elimination half-life of approximately 20 hours to facilitate once-daily dosing. While meloxicam achieves steady-state plasma concentrations within 3 to 5 days, its Tmax—the time to reach peak concentration—can range from 5 to 11 hours, making it unsuitable for immediate acute pain relief.
As noted by Doctronic experts, “Your choice depends on whether you need sustained relief for ongoing inflammation or quick action for sudden pain episodes.” Clinicians must weigh the pharmacological profiles of these agents against patient safety, as there is a strong imperative to avoid therapeutic overlap. Combining meloxicam and ibuprofen significantly exacerbates the risk of gastrointestinal complications, including stomach ulcers and bleeding, as well as potential nephrotoxicity. While meloxicam is preferentially selective for COX-2, which may reduce stomach irritation compared to non-selective agents like ibuprofen, the combined burden on the kidneys and the cardiovascular system remains a primary clinical concern. Consequently, patients should be reassessed regularly to ensure the lowest effective dose is utilized for the shortest duration necessary, with ongoing monitoring for long-term safety.
Summary Table: Onset, Peak, and Duration Comparisons
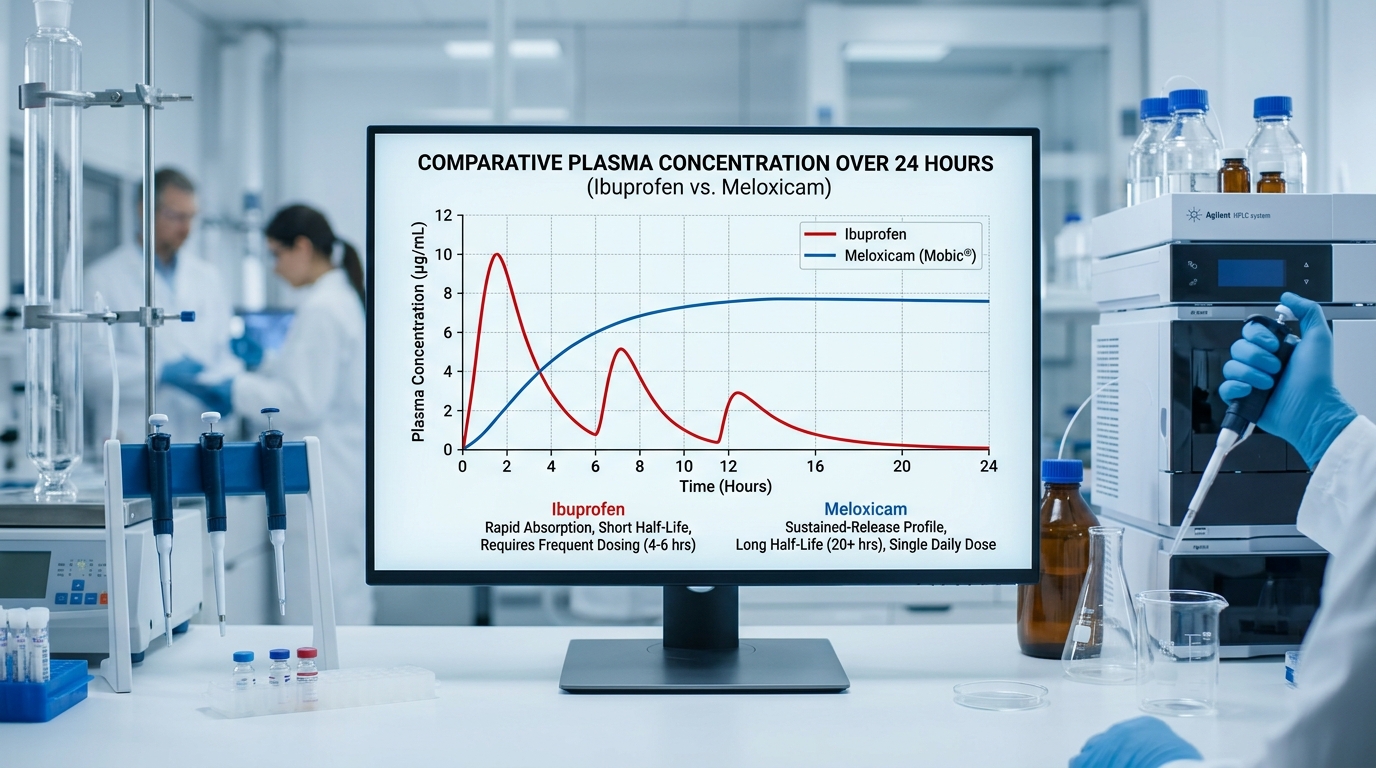
When navigating pain management strategies, understanding the pharmacokinetic distinctions between ibuprofen and meloxicam is essential for clinical decision-making. While ibuprofen has long served as the standard for acute pain due to its rapid onset—reaching a median peak plasma concentration (Tmax) of roughly 0.4–1.3 hours—meloxicam is engineered for sustained efficacy, typically reaching its Tmax in 5–6 hours according to clinical pharmacokinetics data. This slower onset reflects meloxicam’s evolution as a treatment designed for chronic inflammatory conditions, facilitating once-daily dosing to improve patient adherence.
The following table synthesizes these key metrics to assist in treatment planning:
| Metric | Ibuprofen | Meloxicam |
|---|---|---|
| Onset of Relief | 30–60 minutes | Delayed (hours) |
| Tmax (Peak) | 0.4–1.3 hours | 5–6 hours |
| Duration of Effect | 4–6 hours | 24-hour coverage |
| Half-Life | ~2 hours | ~20 hours |
As clinicians pivot toward managing arthritis with long-term therapy, they often prioritize the consistent 24-hour coverage provided by meloxicam, as detailed in our guide to Meloxicam 101: Your Daily Guide to Steady Joint Relief. However, it is vital to emphasize that these drugs function differently: meloxicam’s preferential COX-2 selectivity may reduce gastric irritation compared to non-selective NSAIDs like ibuprofen. Regardless of the choice, practitioners must remain vigilant regarding cardiovascular and renal risks, ensuring patients adhere to the lowest effective dose for the shortest possible duration. Crucially, clinicians must warn patients that combining these agents significantly heightens the risk of severe gastrointestinal bleeding and kidney damage.


