Is Meloxicam Addictive? Understanding the Facts
By Frankie Sze | 5/2/2026
The Origin of the Concern: Why Prescription Status Triggers Addiction Fears
The shadow cast by the opioid crisis has understandably altered the collective patient psyche. In recent years, any prescription medication labeled for pain management often triggers immediate anxiety regarding potential chemical dependency. However, it is essential to distinguish between the clinical necessity of pain management and the physiological reality of addiction. As noted by medical experts, “Patients frequently wonder whether meloxicam or ibuprofen works better for arthritis pain, how quickly each provides relief, and how often they must be taken;” source, reflecting a broader, valid concern for safety in an era of medication caution.
Meloxicam stands as a critical distinction in this landscape. As a non-steroidal anti-inflammatory drug (NSAID), it is fundamentally distinct from narcotics or opioids. The FDA prescribing information for meloxicam explicitly states in Section 9 that there is no clinical evidence of abuse or dependence, making it a cornerstone for millions of adults managing chronic arthritis. While patients may experience what feels like a return of symptoms—often termed ‘rebound pain’—when stopping treatment, this is merely a return of original inflammation rather than the hallmark of chemical withdrawal. For those seeking consistency in their management routine, Meloxicam 101: Your Daily Guide to Steady Joint Relief provides a comprehensive overview of how this medication fits into a modern, non-addictive treatment regimen.
While meloxicam is widely prescribed and free from the addiction risks associated with opioids, it remains a potent pharmacological agent that requires careful oversight. It is typically dosed once daily at 7.5 mg to 15 mg to balance efficacy with safety. Furthermore, patients must remain aware of specific contraindications, such as the necessity to avoid NSAIDs after 20 weeks of pregnancy due to risks including reduced amniotic fluid. Looking toward the future, ongoing research into COX-2 selectivity suggests that we are moving toward even safer NSAID formulations with reduced gastrointestinal risks, ensuring that patients can find relief without compromising their long-term health.

Mechanism of Action: Prostaglandins vs. Brain Reward Pathways
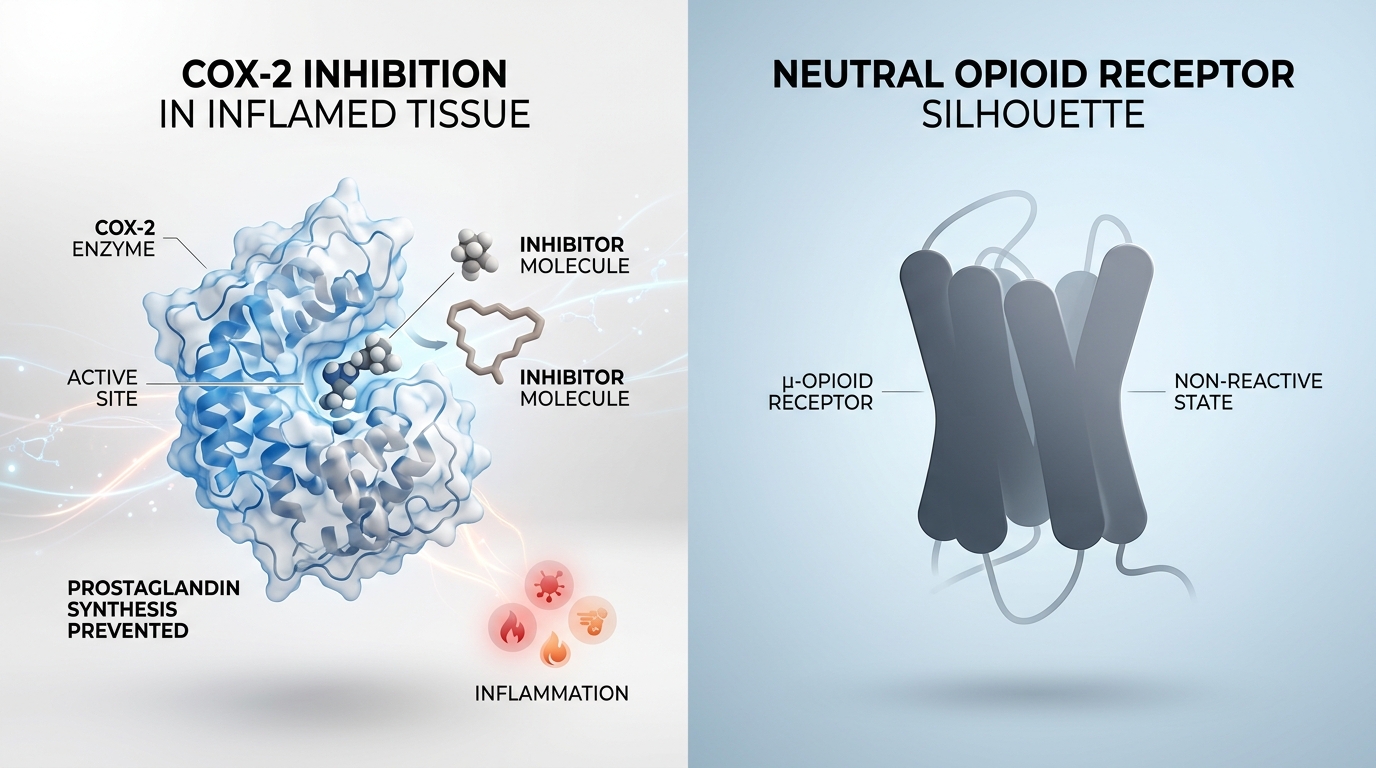
In an era shaped by the profound toll of the opioid crisis, clinicians and patients alike remain understandably vigilant regarding the potential for dependence in pain management. Meloxicam, a potent non-steroidal anti-inflammatory drug (NSAID) typically dosed at 7.5 mg to 15 mg once daily, serves as a critical, non-addictive alternative for millions of adults suffering from arthritis. Unlike narcotics, which target the brain’s reward centers, meloxicam exerts its effects primarily through the inhibition of cyclooxygenase (COX) enzymes, thereby reducing the production of prostaglandins that signal inflammatory pain at the site of injury. As noted by experts in pharmacological recovery, “Unlike opioids, meloxicam does not interact with the central nervous system in the same way, eliminating the potential for a euphoric high.”
This distinct mechanism is further supported by clinical data; the FDA prescribing information in Section 9 explicitly states there is no evidence of abuse or dependence associated with the medication. While some patients report “rebound pain” upon discontinuation, it is imperative to distinguish this clinical phenomenon from chemical withdrawal. The return of discomfort is merely the re-emergence of underlying inflammation as the systemic drug concentration wanes, rather than a physiological craving driven by neurochemical changes in the brain. Despite its safety profile regarding addiction, clinicians must exercise caution in specific populations, as NSAIDs should be avoided after 20 weeks of pregnancy due to risks such as reduced amniotic fluid. Looking toward the future, ongoing research into COX-2 selectivity suggests the next generation of NSAIDs may offer even greater safety profiles, further distancing the therapeutic approach to chronic pain from the pitfalls of narcotics.
Medical and Legal Classification: Why Meloxicam is Not a Controlled Substance
In an era shaped by the profound trauma of the opioid crisis, patients and clinicians alike are understandably cautious regarding any pharmacological intervention for pain. However, medical and legal frameworks clearly distinguish meloxicam from narcotic and opioid analgesics. As a non-steroidal anti-inflammatory drug (NSAID), meloxicam works primarily by inhibiting cyclooxygenase enzymes to reduce inflammation, a mechanism entirely distinct from the central nervous system pathways targeted by addictive substances. Confirming this regulatory status, the U.S. Drug Enforcement Agency (DEA) has not officially classified meloxicam as a controlled substance.
The safety profile of the medication is further substantiated by clinical documentation. According to the FDA prescribing information, Section 9 explicitly confirms there is no evidence of abuse or physical dependence associated with its use. For millions of adults managing chronic conditions such as arthritis, this makes meloxicam a vital, non-addictive alternative to stronger narcotics. Patients typically follow a simple once-daily dosing regimen of 7.5 mg to 15 mg, and while some may experience ‘rebound pain’—a return of the original underlying inflammation—upon cessation, this is a physiological symptom of the returning condition rather than the chemical withdrawal seen with controlled narcotics.
While meloxicam provides significant relief for many, its usage requires professional oversight. Medical guidance dictates that NSAIDs should be avoided after 20 weeks of pregnancy due to risks such as reduced amniotic fluid, which can impact fetal development. As we look toward the future, ongoing research into COX-2 selectivity continues to inform the development of safer NSAID formulations, aiming to mitigate gastrointestinal risks and further solidify the role of non-opioid options in chronic pain management.
Misuse vs. Dependency: The Risks of Overuse Without the High
In the shadow of the opioid crisis, the public has understandably developed a heightened anxiety surrounding any prescription pain management. However, it is clinically vital to distinguish between the neurobiological craving associated with addiction and the physiological risks of medication misuse. Meloxicam, a potent non-steroidal anti-inflammatory drug (NSAID), is a cornerstone of modern arthritis treatment precisely because it operates outside the pathways of narcotics. As noted in the FDA prescribing information, Section 9, there is no evidence of abuse or dependence associated with its use, even when prescribed at the standard once-daily dosage of 7.5 mg to 15 mg.
As Ikon Recovery Centers clarifies, “Neither meloxicam nor ibuprofen is considered addictive, though both carry risks of serious side effects when misused or taken in excessive amounts.” While meloxicam does not produce the chemical dependency seen with opioids, it is not without peril. Patients often mistake the return of original inflammation—known as ‘rebound pain’—for withdrawal symptoms. Unlike narcotic withdrawal, this is simply the pharmacological effect wearing off, allowing the underlying inflammatory condition to reassert itself.
The risks of overusing meloxicam are not behavioral, but systemic. Indiscriminate dosing can lead to severe gastrointestinal, renal, and cardiovascular complications, necessitating a careful balance. Furthermore, clinical caution is paramount during pregnancy; NSAIDs like meloxicam should be avoided after 20 weeks of gestation due to significant risks, such as reduced amniotic fluid levels. Looking toward the future, ongoing research into COX-2 selectivity promises a horizon of even safer NSAID formulations designed to minimize these gastrointestinal vulnerabilities, ensuring that meloxicam remains a reliable, non-addictive tool for millions navigating chronic pain.
Stopping Meloxicam: Distinguishing Rebound Inflammation from Withdrawal
In an era shaped by the opioid crisis, patients are understandably cautious regarding prescription pain management. However, it is clinically vital to distinguish between physical dependence and the pharmacological action of meloxicam. As a non-steroidal anti-inflammatory drug (NSAID), meloxicam is not a narcotic or opioid, and the FDA prescribing information in Section 9 explicitly confirms there is no clinical evidence of abuse or dependence associated with the medication. While meloxicam is widely prescribed for millions of adults as a safe, non-addictive alternative to stronger analgesics, cessation must be handled with an understanding of its mechanism of action.
Because meloxicam is typically dosed once daily at 7.5 mg to 15 mg to suppress systemic inflammation, stopping the medication does not induce the chemical withdrawal symptoms seen in addictive substances. Instead, individuals may still experience discomfort and a return of inflammation, often referred to as “rebound pain,” when discontinuing the medication. This phenomenon represents the resurgence of the patient’s underlying arthritis symptoms, which were previously masked by the drug’s anti-inflammatory efficacy, rather than a physiological withdrawal. Patients should also note that while future research into COX-2 selectivity aims to further minimize gastrointestinal risks, clinical caution remains paramount; for instance, NSAIDs like meloxicam must be strictly avoided after 20 weeks of pregnancy due to the risk of reduced amniotic fluid. If you feel your symptoms returning, consult your physician to manage the transition rather than assuming the drug has caused a dependency.
Empowered Pain Management: Using Meloxicam Safely and Responsibly
In an era where the shadow of the opioid crisis has understandably led to heightened anxiety surrounding pain management, it is vital to distinguish between medication classes. Meloxicam is a non-steroidal anti-inflammatory drug (NSAID), not a narcotic or opioid. In fact, according to FDA prescribing information, there is no evidence of abuse or dependence associated with its use, making it a reliable, non-addictive alternative for millions of adults managing arthritis. If you are starting your journey with this medication, our Meloxicam 101: Your Daily Guide to Steady Joint Relief offers further insights into maintaining consistent therapeutic levels.
Safety and responsibility remain the pillars of effective treatment. While meloxicam is typically dosed once daily at 7.5 mg to 15 mg, patients should be aware that stopping the medication may result in ‘rebound pain.’ It is important to recognize that this is a return of original inflammation rather than physical withdrawal. Furthermore, pregnancy requires heightened caution; as noted in clinical guidance, “NSAIDs should be avoided in pregnant women at around 20 weeks or later in pregnancy” due to the risk of reduced amniotic fluid levels. Patients should also monitor for signs of allergic reactions, such as rashes or difficulty breathing, and report them immediately to a provider.
Looking toward the future, ongoing research into COX-2 selectivity promises the development of even safer NSAID formulations with reduced gastrointestinal risks. By remaining informed and maintaining open communication with your healthcare team, you can manage chronic discomfort with confidence, knowing you are using modern medicine safely and effectively.


