
Waking Up with Morning Stiffness: The Meloxicam Solution
By Frankie Sze | 5/1/2026
The Morning Struggle: Why Arthritis Stiffness Hits Hardest at Dawn
For millions living with arthritis, the transition from sleep to wakefulness is rarely a gentle awakening; instead, it is marked by what clinicians describe as the ‘rusty hinge’ stiffness that many patients experience upon waking (Doctronic Insights). This phenomenon is not merely subjective discomfort but a physiological reality driven by circadian rhythms; specifically, levels of the pro-inflammatory cytokine IL-6 reach their zenith in the morning hours before tapering off throughout the day. Historically, patients reliant on short-acting NSAIDs have struggled because these medications often metabolize and lose efficacy overnight, leaving them unprotected at dawn. To break this cycle, many turn to the sustained pharmacokinetics of meloxicam, which offers a terminal elimination half-life of 15 to 20 hours. As outlined in Meloxicam 101: Your Daily Guide to Steady Joint Relief, initiating a once-daily regimen requires patience, as steady-state concentrations are typically reached only after 3 to 5 days of consistent dosing. While meloxicam reaches initial peak plasma concentrations within 4 to 5 hours—with a secondary peak occurring at 12 to 14 hours—the true benefit of this treatment is cumulative. An 18-month clinical study confirmed that this consistent approach significantly improves morning stiffness and grip strength, offering a path toward regained mobility that short-acting therapies simply cannot match.

The Biological Clock: How Inflammation Peaks While You Sleep
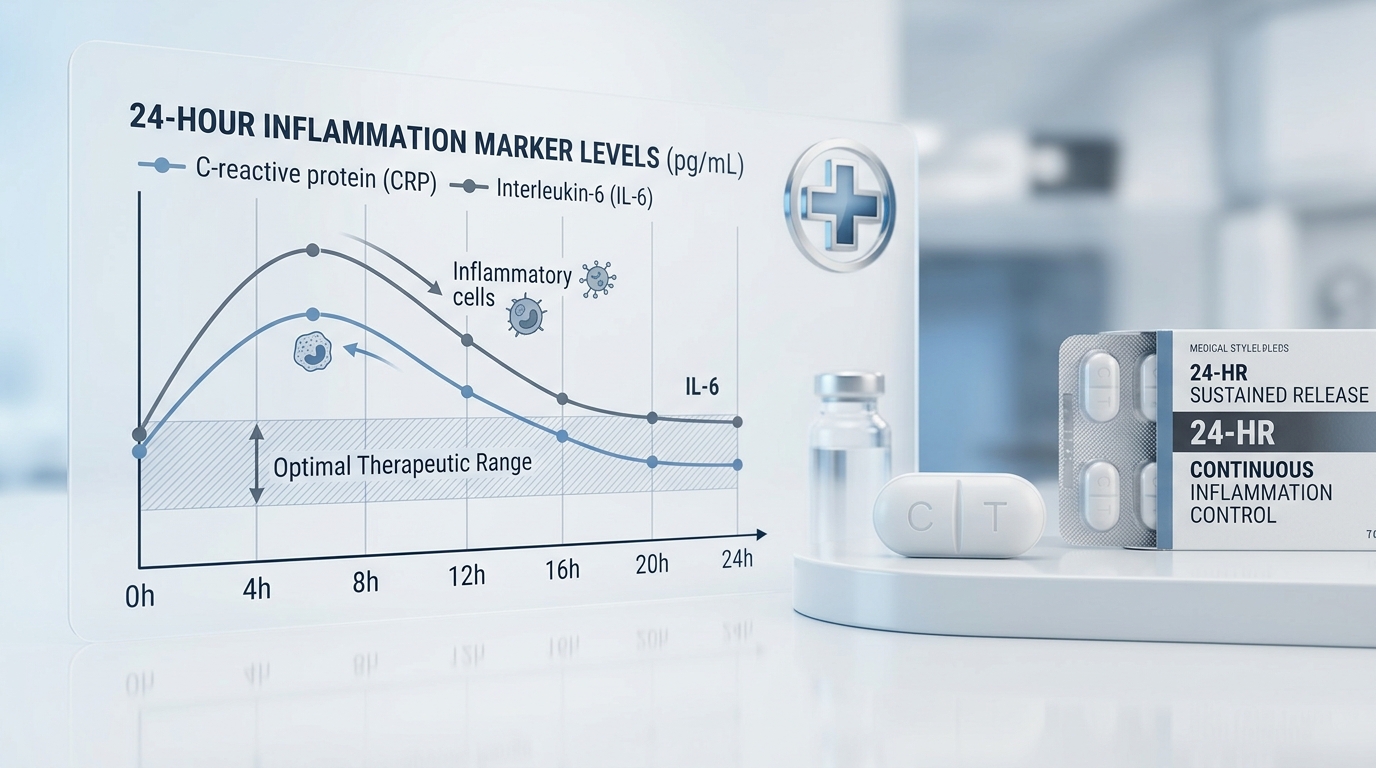
For many living with chronic arthritis, the night is not a time of rest, but the prologue to a painful morning. While patients have historically relied on short-acting NSAIDs, these medications often metabolize too quickly, leaving the body unprotected during the critical predawn hours. The underlying culprit is a disruption in the body’s inflammatory homeostasis; specifically, interleukin-6 (IL-6) levels follow a distinct diurnal rhythm. As noted in research, “Peak values appeared in the morning and low values in the afternoon and evening.” This morning surge in proinflammatory cytokines is exactly why stiffness and grip strength impairment are most pronounced upon waking.
Transitioning to a once-daily regimen of meloxicam offers a strategic pharmacological intervention against this cycle. Unlike traditional NSAIDs, meloxicam possesses a terminal elimination half-life of 15 to 20 hours, providing more sustained coverage. Following ingestion, the medication reaches peak plasma concentrations within 4 to 5 hours, with a secondary peak occurring at 12 to 14 hours—a profile that helps bridge the gap through the night. However, patients must understand that therapeutic consistency is key; steady-state concentrations are typically reached only after 3 to 5 days of continuous dosing. As evidenced by an 18-month clinical study, this dedication to a consistent regimen significantly improves morning stiffness and long-term functional mobility, marking a shift from reactive symptom management to a cumulative, sustainable reduction in inflammation.
Meloxicam’s 24-Hour Shield: Understanding the Long-Acting Difference
For patients managing chronic arthritis, the cycle of pain has historically been dictated by the fleeting efficacy of short-acting NSAIDs. When these medications wear off during the night, they leave patients vulnerable to the intense inflammation that often peaks in the early morning hours, coincident with the natural rise of IL-6 levels. Meloxicam fundamentally alters this landscape by providing a more sustained pharmacological approach. With a terminal elimination half-life of 15 to 20 hours, it bridges the gap that leaves others in pain overnight.
As noted in clinical research, “Meloxicam has a terminal elimination half-life of 15–20 h. Therefore, steady state is achieved after 3–5 days continued treatment” (PMC1884180). This unique pharmacokinetic profile, characterized by peak plasma concentrations 4 to 5 hours post-ingestion followed by a secondary peak at 12 to 14 hours, ensures continuous coverage throughout the day. While patients may experience a delay before reaching full therapeutic concentrations—typically within 3 to 5 days of once-daily dosing—the resulting consistency is transformative. Long-term data, including an 18-month study, confirms that this persistent reduction in inflammation translates to objective clinical benefits, specifically in the alleviation of morning stiffness and the restoration of grip strength, ultimately fostering improved overall mobility.
Timing for Success: Should You Take Meloxicam in the Morning or Evening?
For patients suffering from chronic inflammatory conditions, the dawn is often the most difficult part of the day. Clinical research has established that IL-6 levels in arthritis patients peak in the morning, which correlates directly with the onset of severe joint stiffness and diminished grip strength. While patients have historically relied on short-acting NSAIDs that wear off during the night, leading to painful awakenings, the pharmacokinetic profile of meloxicam offers a more strategic advantage. With a terminal elimination half-life of 15 to 20 hours, meloxicam is designed for stable, once-daily dosing, though it requires a window of 3 to 5 days of consistent use to achieve steady-state therapeutic concentrations.
The key to managing morning symptoms lies in synchronizing the medication’s plasma levels with the body’s inflammatory cycle. Meloxicam reaches its primary peak plasma concentration 4 to 5 hours after ingestion, but it also exhibits a secondary peak at 12 to 14 hours. As noted by clinical insights on meloxicam pharmacokinetics, this drug “exhibits a secondary peak around 12–14 hours, suggesting that an evening dose (taken with dinner) can align the secondary peak with the early morning hours.” By shifting the administration to the evening, patients can effectively utilize this secondary surge to counteract the morning inflammatory spike. An 18-month clinical study confirmed that this consistent long-term use significantly improves morning stiffness and grip strength, providing a clear pathway for improved mobility as steady-state levels are maintained through daily adherence.
Reclaiming Your Morning: Practical Tips for Early Movement
Transitioning from short-acting NSAIDs that often wear off overnight requires a strategic approach to bridge the gap in symptom management. Because IL-6 levels in arthritis patients naturally peak in the early morning, patients frequently endure significant stiffness before their medication takes effect. Meloxicam provides a more consistent profile, with a terminal elimination half-life of 15 to 20 hours, yet it typically requires 3 to 5 days of once-daily dosing to reach steady-state concentrations. Given that the medication reaches peak plasma levels 4 to 5 hours after ingestion—with a secondary peak occurring at 12 to 14 hours—timing your dose is essential to aligning peak efficacy with your morning wake-up time.
For those looking to optimize their regimen, experts at Doctronic note: “You can switch your dosing time by taking your last morning dose, then waiting your normal interval before starting evening dosing. This prevents medication gaps while avoiding double-dosing.” By shifting your dose to the evening, you allow the secondary peak to assist in combating the rise in inflammatory markers that trigger morning pain.
While this transition phase demands patience, the long-term outlook is promising. An 18-month clinical study confirmed that consistent meloxicam use significantly improves morning stiffness and grip strength. As you settle into this routine, pairing your medication with gentle morning movement—such as rhythmic joint range-of-motion exercises—can further assist in recalibrating your body’s rhythm, leading to a cumulative reduction in discomfort and a measurable improvement in overall daily mobility.
Conclusion: Moving Beyond the Morning Wall
For decades, patients burdened by inflammatory joint conditions have been trapped in a cycle of relying on short-acting NSAIDs that inevitably wear off overnight, leaving them to face a harsh ‘morning wall’ of severe pain and stiffness. Transitioning to a once-daily meloxicam regimen represents a shift from reactive to proactive management, though patients must maintain patience during the initial adjustment period. Because meloxicam possesses a terminal elimination half-life of 15 to 20 hours and reaches steady-state concentrations only after 3 to 5 days of consistent dosing, immediate results are not always instantaneous.
Understanding the body’s internal clock is essential to this process; IL-6 levels in arthritis patients typically peak in the early morning and trough in the evening, which is why persistent coverage is critical. Meloxicam provides a unique pharmacokinetic profile, reaching initial peak plasma concentrations 4 to 5 hours after ingestion with a secondary peak at 12 to 14 hours, effectively buffering the systemic inflammatory response. For a deeper understanding of how to optimize your schedule, consult our Meloxicam 101: Your Daily Guide to Steady Joint Relief.
The long-term benefits of this consistency are well-documented. An 18-month clinical study confirmed that the cumulative effect of reducing the cytokine burden leads to tangible improvements in daily function. As noted by researchers in the published findings: “Health status, general condition, morning stiffness, grip strength… all improved significantly. Efficacy was maintained through the study.” By adhering to a steady regimen, patients can move beyond the morning wall, securing improved mobility and a more consistent quality of life.


